Educate. Thrive.Your resource for health and wellness information
|
|
The vast array of available prenatal vitamin options out there are staggering. Whether they are over the counter, or prescription, the quality is broad and often overwhelming. So, where is a pregnant mother to turn? With so many options over the counter, and physicians with mediocre nutritional education, how are they to know what is a good prenatal vitamin and what isn't? Today I am going to tell you why YOUR PRENATAL VITAMIN SUCKS and what you can do about it. So, sit back and grab a cup of tea, because this is going to be a one heck of a ride. Why the Right Prenatal is Important Written by Sarah Thompson Functional Medicine Acupuncturist & Doula Prenatal Nutrition Crash CourseBefore we even begin to discuss the quality and variety of prenatal vitamins, you've got to understand the basics of prenatal nutrition...and some of the more advanced aspects (that even your practitioner doesn't know!). So, what is nutrition? "Well, that's a stupid question Sarah!" Not really. When we generally discuss nutrition, we are talking largely about macronutrients, their ratios and balance, food choices, and occasionally the more common micronutrients as they pertain to energy production (calories). But, there is more...oh, so much more. Nutrients are cofactors in many of the biological processing in the body: They fuel and initiate neurotransmitter and hormones formation and function; they regulate cellular division; they regulate the expression of genes; they keep your body functioning at it's finest. If there are deficiencies, or imbalances in nutrients the body cannot function properly. In order to choose a quality prenatal vitamin, we must understand how these nutrients work on a biochemical level. Each trimester needs specialized nutrition. THERE IS NO ONE SIZE FITS ALL PRENATAL VITAMIN. There I've said it. I've gotten it out in the first few paragraphs. There is no single vitamin that will fill all your needs from conception through lactation. In fact, many nutrients that are essential for conception could hinder the function of your birth, and vica versa. In order to truly know what a prenatal vitamin should have in it, lets dive into this by trimester and look at what is really going on in the body, on a biochemical level. Now, most nutritional deficiencies begin slowly. You don't just develop scurvy overnight. There are stages of deficiency, often with very slight and very dismissable symptoms. Some of which are common pregnancy complaints, such as restless leg and calf cramps. This is why the dietary choices, and the nutritional status leading into pregnancy is probably the most important part of prenatal nutrition. Most nutritional based birth defects and reproductive complications occur in the first 12 weeks of pregnancy, often before someone even knows they are pregnant. In addition, when we see a deficiency, we must go backwards. If you are showing an issue in the first trimester, this is more likely due to poor nutrition prior to conception. If you are having issues in the 2nd trimester, this may be due to poor diet during the first trimester (darn you morning sickness). If you have a difficult labor due to nutritional deficiencies, this is due to poor nutrition leading up to labor. PreconceptionYour nutritional status prior to pregnancy will set you and your baby up for either success or failure through pregnancy, childbirth and beyond. At this phase of pregnancy, we are building a foundation. The majority of women I see at this stage are far more focused on conception, and not on the implications for the pregnancy itself. They just want to become pregnant, they will figure out the rest out as it comes. In prevention of things such as miscarriage and morning sickness, proper preconception nutrition is essential. So, what does this look like? In preconception, our focus is largely on the health of the sperm (yes dad's nutrition plays a big role in this) and the egg. If either of these are nutritionally deficiency, they will be weak and could lead to miscarriage or birth defects. When looking into egg health, we look at a number of considerations. As the egg is developing (9-10 months before release from the ovary by the way), it is being influenced by a number of factors that determine how healthy that egg will be. Vitamin E and Beta Carotene play a large role in this process. Both are powerful antioxidants that have receptors on the ovary. In fact the highest concentration of both are found in the corpus luteum and the adrenals. After ovulation, the corpus luteum is responsible for the production of progesterone in preparation for conception. If the corpus luteum is weak, there will not be enough progesterone to support the embryo until it has implanted in the uterus. Thus causing miscarriage. Vitamin D is technically another steroid hormone. Antimullerian hormone (AMH) is a hormone that is produced by the developing follicle. Vitamin D alters AMH signalling, FSH sensitivity, and progesterone production. Which means it plays a very large role in the health of ovulation and thus the outcomes of conception. Another key nutrient is Zinc. Now, we know that zinc is essential for the health of the egg (and sperm). In fact, thanks to the wonderful work done around IVF, we know that zinc deficiency is a common cause of miscarriage due to a weak connection (sad eggs/sperm) at conception. When the sperm and egg meet there is a literal spark that occurs, this is catalyzed by zinc. Without enough zinc, there is a weak spark and this connection does not result in an embryo. There is, obviously, significantly more that goes into fertility and reproduction than just Vitamin E, Beta Carotene, Vitamin D and Zinc. But for the purpose of this post, we will keep it on a need to know basis of nutrition.
First TrimesterCongratulations! Your pregnant. You've had enough nutritional reserve for a successful conception, so things are probably right where they need to be, right? Usually, but not always. This is the most important time for the outcome of your baby's health. It is the first couple weeks of development where issues can arise. Sometimes nutritional deficiencies during this phase go unnoticed, and sometimes the red flags are in our faces and we just don't see them. The primary focus of mainstream prenatal nutrition is based on fetal development...not maternal health. Unfortunately. Although most of this goes hand in hand, there are sometimes nutritional demands on the mother, that are not on the fetus, and thus not the same requirements. The main focus of nutrition in the first couple of weeks/months, like I said, is primarily on the fetal development when the majority this growth is happening. This is also when most women have morning sickness with poor dietary intakes (which can set you up for other issues throughout pregnancy). Lets take a look at what all is happening at this time, to understand what the nutritional needs are. Vitamin A in the fist trimester has become a bit of a debate. Deficiencies are associated with birth defects, and so are excesses. For more information on this, please read my other blog post "Eating Liver in Pregnancy - Is it Safe?". Vitamin A has been linked to the development of the cardiovascular system (heart), and the central nervous system of your baby and is a crucial part of the prenatal diet. The DNA of your baby is being transcribed. What you do. what you eat. Your emotions. These all tell your baby how to develop. Certain nutrients are necessary for proper DNA transcription in the early phases of pregnancy (as early as conception really). B Vitamins such as Folate, B12, and B6, as well as adequate amino acids (proteins), choline (elevated progesterone stimulates formation of choline from the liver) and betaine (which is found in beets and grains) are necessary for this to occur properly. Other B Vitamins are necessary for fetal development. Riboflavin (Vitamin B2) is necessary for your baby's brain, nerves and muscles to develop. Pantothenic Acid (Vitamin B5) is necessary for the absorption of B2. Niacin (Vitamin B3) is the precursor for a very important chemical called NAD. NAD is needed for many different processes in the body, and is essential in fetal development. It is also needed for the synthesis of the steroid hormone of pregnancy. Your baby's brain is also developing at this time. Nutritional fats, such as DHA are essential for healthy development as are B vitamins, such as Folate, and B12, Iron for myelination of nerves, Zinc for Autonomic NS development, and others such as Copper, Iodine, Selenium, Vitamin A, and Choline. At this point the placenta is also developing. This is a very important part of early pregnancy. Issues in the development of the placenta could lead to issues such a fetal growth restriction and gestation hypertension if the blood vessel are developed too narrow. For more on this please read my other blog post on "Preventing Preeclampsia". In order for the placenta to form properly you need adequate amounts of Vitamin A to stimulate the production of Vitamin D receptors, Vitamin D for the formation of several enzymes produced by the placenta in development. Magnesium for the proper development of blood vessels in the placenta and uterus. Vitamin K to prevent hemorrhaging as the placenta and uterus form. Progesterone is the highest it will ever be, and the body is turning over serum progesterone every 20 minutes. Progesterone needs adequate amounts of Vitamin E, Vitamin D, Iron and dietary cholesterol to be made properly. In this initial development of both the placenta and the fetus, mitochondrial health is of upmost important. Several nutrients go into the health and function of the cellular mitochondria; B Vitamins, Vitamin E, Coenzyme Q10, Vitamin C, Zinc, Selenium, L-Carnitine.
Second TrimesterThis is typically the smooth sailing period of pregnancy. The placenta has been well established and is taking over (which means your baby is no longer living off of nutritional stores, but off your diet), and you have a pretty well developed little fetus with all its organs in place. From here through the 3rd trimester there are still some growth going on, on the part of both you and baby. Baby is growing in size, which requires adequate amounts of protein, minerals (magnesium, phosphorus, calcium), and Vitamin D and K2 for muscle and bone development. Your baby's brain is also developing still. It requires adequate amounts of nutritional fats, such as DHA, as well as B Vitamins like B12, folate, and B6, Zinc, Selenium, Iodine and Choline to develop healthy neurological connections. Your amniotic fluid levels are rising and filtering, meaning that you need constant replenishing through fluid intake, electrolytes (Magnesium, Potassium, and Sodium) and antioxidants. Vitamin C and Vitamin E make up the majority of antioxidants in the amniotic fluid with the job of preventing the cytokines being produces by the developing fetal lungs from causing labor too early. For more on this please read my other article, "Amniotic Fluid Health in Childbirth Outcomes." Another very important change in your body is the amount of blood volume that is being produced. During the 2nd trimester, the amount of blood volume has to double in order to fill the needs of both you and baby. In order to do so, adequate nutrition is needed. This includes Iron, Copper, Zinc, B Vitamins (B6, Folate, B12), and Vitamin A. A deficiency in any of these nutrients can cause anemia...not just iron deficiency.
Third TrimesterMuch of what I have already discussed has been addressed before. Many of you already know of the nutritional demand the fetus takes, as well as the nutritional demand of conception. But, how many of you know the nutritional demands of childbirth? The third trimester is when you prepare, nutritionally, for childbirth. I've written another blog series on this topic, and will link over to relevant entries. As we prepare for labor, several things are going to happen, and this where nutrition changes. The same prenatal vitamin that you used in early pregnancy, isn't going to be your best bet for childbirth. You child is pretty well developed, with only a few things needing to grow (size, lungs...). This of course requires the same nutritional needs as the second trimester. As we enter the last month of pregnancy severally things are happening with your body. Childbirth nutrition is usually something we want to start addressing around 30-34 weeks. Oxytocin receptors are being formed, and oxytocin production is beginning in the brain. Oxytocin formation require adequate amounts of protein, and the receptors need adequate amounts of vitamin A to be made. Once the receptors are formed and oxytocin is made, in order to initiate contractions in labor, there needs to be adequate Magnesium, and Cholesterol in order for the receptor on the uterus to cause a contraction. For more on this please read my article, "Oxytocin, the Elvis of Childbirth." The other cool thing that is happening, is that elevated levels of estrogen are causing changes in your cervix. This elevated level of estrogen is responsible for the formation of oxytocin receptors, prostaglandins, hyaluronic acid, and blood clotting agents. In order make these changes happen there needs to be an abundance of certain dietary components; Vitamin A, Linoleic Acid, Saccharides, Iron. For more information on how cool cervical ripening is, please read by article, "Cervical Ripening; The Key to Natural Labor." **There will be an additional post of postpartum of lactation nutrition**
The "America is so Cool, that Nutritional Deficiencies are Rare" MythSo, we've discussed the basics of prenatal nutrition. But this is America, nutritional deficiencies are rare, right? I am sure you have read or heard this before. Here in America, with the food fortification system, we've wiped out nutritional deficiencies. I hate to be the one to drop the pot here, but this is a myth. According to the CDC the majority of American are eating a nutrient poor diet.
Based on the data collected by the CDC, the Health and Nutrition Examination Survey showed that Americans aren't doing so well...
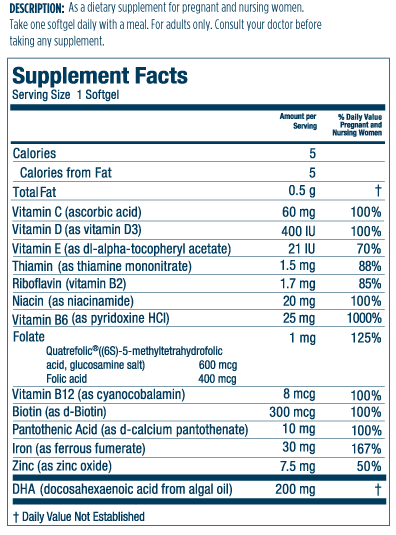
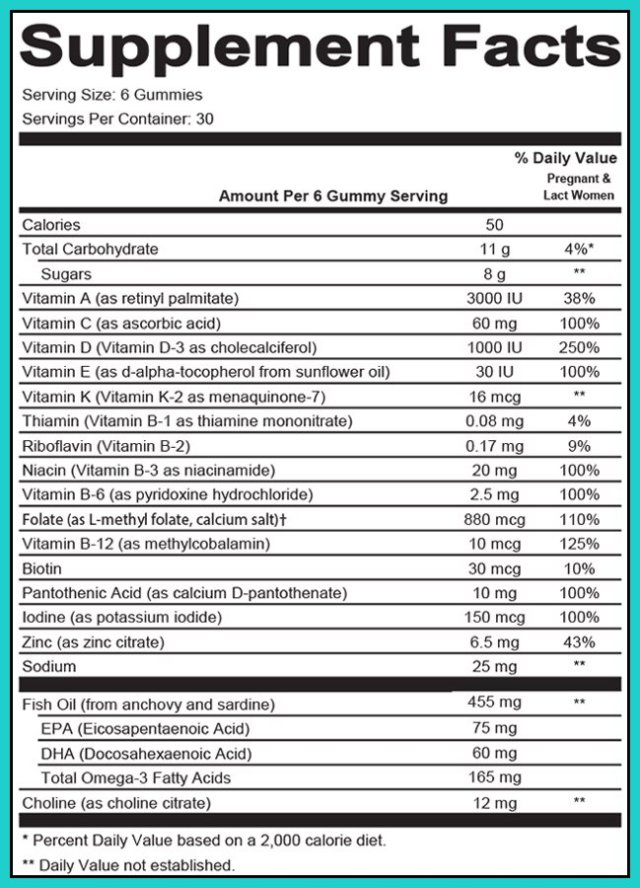
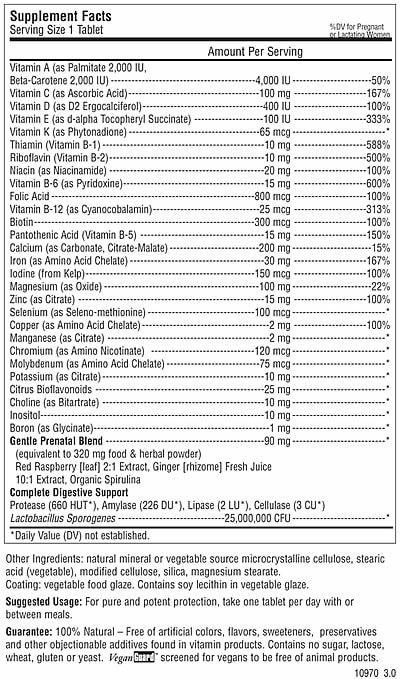
...and it's only worse in pregnancy. Let that sink in......................................................................... Vitamin E and Vitamin D are required for healthy ovulation, and over 90% of Americans are not consuming enough! Vitamin A is essential for conception, fetal development, oxytocin function, and over 50% are deficient. Magnesium is necessary for Oxytocin function, and muscle health (your uterus is just a big muscle, right?) and 60-90% of the population is deficient. Vitamin C helps prevent preterm labor, and over 40% of the population is not consuming enough. (I've actually seen this one pop up in lab testing and patients are always shocked). Dietary fats are necessary for the production of prostaglandins and fetal brain development, and 60% of Americans are not getting enough. Another common cause of nutritional deficiencies in women of reproductive age is the use of contraceptive birth control. Many cause nutritional deficiencies (largely B Vitamin and Electrolyte) that can take months/years to recovery from post use. For more information on your specific birth control method and how it affects nutritional status, email me. What Do I Look for In a Prenatal VitaminThere are so many changes that occur during conception and pregnancy, and thus there is not a single prenatal vitamin that is best for the entire pregnancy, or fertility through lactation for that matter. Each period of gestation has a different need, and thus a different prenatal need. Of course, when choosing a prenatal vitamin your diet also must be considered. By looking closely at what you are eating, dietary philosophies (vegan), medical history (celiac, thyroid, PCOS) and your symptoms, supplements in addition to a basic prenatal may be necessary to bring levels to adequate amounts...if only there were customizable/compounded prenatal vitamins based on your specific needs, wouldn't that be something. Vitamin A: In conception and the first trimester, YOU NEED VITAMIN A. Contrary to what the poor research studies relay. When I am looking at a prenatal vitamin for conception and the first trimester, I avoid Retinyl Palmitate Vitamin A in supplements. This is the form associated with birth defects if too much is consumed. You are safe if you stick with a Beta Carotene, as this is converted as needed to the retinoid forms, so there is no risk of over supplementation. Now, in the later gestation, and in preparation for childbirth, I want to see that Retinyl Palmitate (or the addition of liver in the diet). Vitamin A in the Retinoic Acid form is what is required for the formation of oxytocin receptors. Any deficiency in the retinoid form at this point in gestation could have a negative effect on the outcomes of childbirth. The risk of birth defects is no longer an issue, as the period (conception, first trimester) of neurological development is complete. This is what I was speaking of when I said that nutrition at the beginning and the end of pregnancy are quite different, and cannot be treated the same without negative effects. I've seen several prenatal vitamins with ZERO Vitamin A in them for fear of potential birth defects. This is at the detriment of you, the pregnant mother, and possibly your developing baby. Dosage preconception - 2nd trimester: 1500mcg-3,000mcg/4000iu - 8,000iu in the Beta Carotene Form only Dosage 3rd trimester: 1500mcg/4000iu in a Beta Carotene + Retinyl Palmitate Mix Vitamin C: Vitamin C is a potent antioxidant, and is needed for Vitamin E to function properly. Adequate amounts are needed throughout pregnancy. In the amniotic fluid, both Vitamin C and E prevent preterm labor. As we near labor though, too much can actually cause a delay in labor initiation. Labor is an inflammatory reaction, and antioxidants in supplement form may reduce inflammation too much. So a small decrease in the amount of Vitamin C is what I like to see at this stage. Dosage preconception - 2nd trimester: 350-500mg Dosage 3rd trimester: 100-120mg Vitamin D: Vitamin D is essential through conception and breastfeeding, especially in the winter months. In fact an additional vitamin D supplement may be used if pregnancy is during the winter. When choosing a prenatal I look for the cholecalciferol (D3) form of Vitamin D. This is the form that is naturally produced in the body, and thus the preferred form. There is conflicting research on the effectiveness of ergocalciferol (D2) in the adequate raising of functional vitamin D levels in the blood. Dosage: 25-50mcg/1000-2000iu Vitamin E: Like Vitamin C, Vitamin E is a potent antioxidant. In addition it plays a critical role in progesterone products and is essential in conception and early pregnancy. Throughout pregnancy, it is necessary for the prevention of preterm labor. Again, too much, just like vitamin C, can cause a delay in the natural initiation of labor. I like to see less in a late term prenatal vitamin. Dosage preconception - 2nd trimester: 50-100mg Dosage 3rd trimester - 20-40mg Vitamin K: As we discussed, the role of Vitamin K in blood clotting is essential and is primarily controlled by the K1 form. Vitamin K2 is used in the utilization of Vitamin D3 in the formation of bone in your growing fetus and also has blood clotting capabilities. Adequate amounts of Vitamin K are needed through pregnancy in the prevention of hemorrhagic conditions. It is a long standing myth that Americans consume enough vitamin K in their diet. Did you know that the vitamin K in spinach is only 10% absorbable? Vitamin K2 found in fermented foods and animal products is more absorbable. The RDA for Vitamin K is not accurate, and many studies suggest that 90+% of Americans don't consume enough and are deficient. Often, with patients who have made the decision to not administer the Vitamin K shot to their newborn at birth, we will increase dosage with an additional supplement. (this is to be cautioned and discussed with your primary care provider.) When choosing a prenatal, I like to see a Vitamin K2, since it is more readily absorbed, with more closer to labor. Dosage preconception - 2nd trimester: 50-100mcg 3rd trimester: 100mcg Thiamin (Vitamin B1): I didn't touch too much on this vitamin, but like all the B vitamins it is essential in mitochondrial health, and more importantly the conversion of carbohydrates and fats into ATP energy. In one study, 30% of pregnant women tested had a measurable B1 deficiency. Dosage: 3-5mg Riboflavin (Vitamin B2): We discussed its importance for neurological development of your baby in the first trimester. A deficiency also predisposes you to a higher risk of preeclampsia. Deficiency is much more common in vegans, and vegetarians who do not consume enough dairy and eggs. I would want to see more in the conception/first trimester phase and more so in those who have been or are vegan during their pregnancy. Dosage preconception - 1st trimester: 10+mg (20mg in vegans) Dosage 2nd trimester - 3rd trimester: 3-5mg Niacin (Vitamin B3): Like all the other B vitamins it plays a role in mitochondrial function, as well as carbohydrate and fat metabolism into ATP energy. In addition niacin is needed in the metabolism of amino acids into neurotransmitters, and in the synthesis of steroid hormones (estrogen, progesterone). B3 deficiency is linked with miscarriage. I like to see this in the niacinamide form, as it is more usable. Dosage: 20-25mg Pantothenic Acid (Vitamin B5): B5 is necessary for the use of B2. Most B vitamins need each other to either absorb or to function, so a complete B complex in a prenatal is a must. B5 is also essential for mitochondrial health, and in the conversion of carbohydrates and fats into ATP energy. It is also necessary for the metabolism of cholesterol which is needed for all those hormones and the oxytocin receptors to function properly. I like to see an adequate amount throughout pregnancy. Dosage: 10mg (give or take) Pyridoxine (Vitamin B6): The active form of B6 is actually called pyridoxal-5-phosphate. B6 is critical for conception and first trimester nutrition. I like to see a good amount in the P5P form or a mix of Pyridoxine HCL and P5P, especially in the conception and first trimester phases. P5P has the ability to be an aromatase inhibitor, meaning it also blocks the enzyme that signals estrogen synthesis. Too much of this form of B6 at the end of pregnancy can cause a deficiency in the amount of estrogen being produced. This in turn could cause a deficiency in the cascade of processes that rely on the adequate amount of estrogen (oxytocin receptor formation, prostaglandins, hyaluronic acid, blood clotting...). In addition p5P is needed for the proper synthesis of the neurotransmitters needed for labor and delivery, such as DMT and Dopamine. In a late term prenatal I like to see smaller amounts of a mix of the two forms, especially if there is a history of depression and neurotransmitter imbalances. B6 deficiency is often a cause of severe morning sickness. Dosage preconception - 2nd trimester: 15-20mg Dosage 3rd trimester: <10mg Biotin (Vitamin B7): This is not a commonly mentioned B vitamin, but as your baby begins to develop, this vitamin is important for the correct development of skin, hair and nails, among other things. 30% of pregnancy women will be biotin deficient despite adequate intake. Dosage: >30mcg Folate (Vitamin B9): Folate not Folic Acid. Please choose a prenatal with Folate, and preferably methylfolate. MTHFR is a gene that methylates folate. It is estimated that 50% of the population has some form of MTHFR genetic mutation that limits the body's ability to methylate adequate amounts of folate. This is why I like the methylfolate form. Folic acid is not a naturally formed vitamin, it is a synthetic. Recent research has shown that folic acid is not well used in the body, and may be linked to increased risk of autism. Folate is essential for neurological formation in early pregnancy. Adequate amounts of methylfolate should be seen in a prenatal for conception and early pregnancy. Dosage: 500-1000mcg Cobalamin (Vitamin B12): Like folate, I like to see this in the mehylcobalamin form. B12 is essential for early neurological development. As we enter the second trimester, B12 is necessary for the formation of blood cells. Deficiency is sometimes associated with numbness and tingling in pregnancy (carpal tunnel). Dosage: 200-500mcg Choline: It is estimated that 95% of pregnant women do not consume adequate amounts of choline in pregnancy. I've seen several prenatal vitamins come across my desk that have ZERO choline in them. Without enough choline there can be hindrance in gene expression. It is often thought that because our body makes some of its own Choline, that dietary intake is not necessary. This is incorrect. In fact, new prenatal vitamin "guidelines" (there are no regulations) call for the addition of choline in prenatal vitamins. Dosage: 200-300mg Calcium: With 50-80% of women of reproductive age not consuming enough calcium, making sure your prenatal has adequate calcium is important. You are growing a baby, and that requires adequate amounts of calcium. If you don't have enough, you will become deficient leading to your own bone and teeth issues, among others. Calcium deficiency is associated with an increase risk of preeclampsia as well, and blood clotting issues. I like a combo of Calcium Citrate-Malate. This combo increases abortion 6-9x that of citrate alone. Make sure there is Vitamin D and Magnesium in combination for proper utilization. Dosage: 100-400mg Iron: I've seen so many prenatal vitamins that contain no iron. There is also some fear about giving too much Iron. General Iron deficiency is only about 10%, but Iron deficiency in pregnancy is a bit more common (average 18%). With an increase over gestation (1st trimester - 6.8%; 2nd trimester - 14.3%, 3rd trimester 28.4%). Iron is the cofactor of enzymatic conversion of cholesterol into steroid hormones (progesterone and estrogen), as well it is needed for oxygenation of both mom and baby. I like to see Iron in a prenatal. Adequate blood testing should be used as well to monitor iron levels. An additional iron supplement may be needed. Heme based iron is the most absorbable form (animal based), and non-heme iron (plant based) being poorly absorbed (mostly due to the content of oxalates in plants containing iron, but this is a whole other topic). In a supplement I like to see ferrous biglycinate instead of ferrous sulfate. The biglycinate form has less digestive upset, and is more readily absorbed. Dosage: 20-30mg Iodine: Sadly, many prenatal leave this important trace element out of their formulas. Although iodized salts decreased extreme iodine deficiency symptoms such as goiter, this is a deficiency that is probably more common than we think. It's a bit complicated, but it has to do with the periodic table. Iodine is a halogen, and so is bromide (a chemical used in the processing of grains). Iodine receptors and other processes that use iodine have an affinity for all halogens. Excess intake of bromide, through grain consumption, blocks iodine action. (other very common halogens include Chloride and Fluoride, I think you know these guys). From 1971-2001 Iodine intake in the US dropped 50% (on top of all the contributing chemicals that inhibit iodine function). Iodine deficiency in pregnancy can lead to postpartum hypothyroid, as well as neurological issues in babies (it is associated with reading issues in childhood). The American Academy of Pediatrics and the American Thyroid Association have each released (among other agencies) recommendations on prenatals including iodine in formulation. Iodine testing is mediocre at best, and thus there is not an adequate estimate of iodine deficiency. Iodine should be in the Potassium iodine form. Dosage: 150mcg Magnesium: I cannot tell you how many prenatal vitamins I have seen lacking Magnesium! It is actually quite disturbing to me considering 60-90% of American are not getting enough, and that Magnesium is ESSENTIAL for childbirth. Again, prenatal nutrition is geared towards your developing baby, not your functional maternal health. Magnesium should be in every prenatal vitamin throughout pregnancy. If I see a prenatal without it, that's a garbage vitamin. Also, form is important. If you see Magnesium citrate, that's a glorified laxative and has little functional value. I look for Magnesium biglycinate or a biglycinate-malate combo. A common sign of magnesium deficiency is calf cramps. You know what I'm talking about, and many of you probably have them right now. This is a symptom that is often dismissed by your primary care as a common "complaint" of pregnancy. When in reality this is a sign of imbalance and dysfunction. Your uterus is a giant muscle, that has to efficiently contract during labor. If you enter labor with a Magnesium deficiency, not only will your oxytocin receptors not be able to function properly (remember up top), but think of what is happening to your calves...your uterus is going to do the same thing. It is going to contract dysfunctionally. This can lead to complications in labor, as well as more intense labor contractions. Also...put the Natural Calm powder away. This is not a good product. They just had a really good method of delivery and marketing team. Dosage preconception - 2nd trimester: 125-250mg Dosage 3rd trimester: 250mg-350mg Zinc: Another important mineral throughout pregnancy. Make sure there are adequate amounts throughout. A bit more during conception is important for egg health and embryo formation. Sometimes an addition zinc during this time is required. Zinc deficiency has been linked to postpartum depression, preterm labor, and preeclampsia. I like to see a Zinc Biglycinate as it is more absorbable. Dosage: 10-20mg Selenium: Selenium is most important in the preconception and the 1st trimester (when the fetal heart is developing) through 2nd trimester phases of pregnancy. Selenium deficiency can make iodine deficiency worse. Selenium concentrations in food are dependent on the amount found in the soil. I like to see a moderate amount of selenium in one of the more naturally absorbed forms, such as a yeast derivative and avoid Selenium Selenite which adversely interacts with other vitamins, such as vitamin C. Dosage preconception -1st trimester: 60-100mcg Dosage 2nd trimester - 3rd trimester: 60-70mcg Copper: Although excess copper can deplete zinc, copper should naturally increase during pregnancy. Copper is necessary for the proper developement of your baby in the 1st trimester and blood volume to double in the 2nd. Excess copper postpartum is associated with an increased risk of postpartum depression, so I like to see less copper or no copper in a postpartum supplement. (I plan on writing another blog post on postpartum supplements, as this post is huge). I look for a Copper Biglycinate Chelate. Dosage: 0.5-0.75mg Chromium: Chromium is a trace mineral needed for insulin regulation. Deficiency is associated with gestational diabetes. This is more important in preconception prenatals in patients with PCOS or other insulin issues, and for these patients throughout pregnancy. Chromium deficiency is more common in diets high in refined carbohydrates as this promotes chromium deficiency and elevates blood glucose. Higher dosage of Chromium should be used in those with insulin regulatory issues, or a history of high carbohydrate diets. Preconception dosage for PCOS: >150mcg Dosage: 30-45mcg Manganese: Manganese is the precursor to one of the critical antioxidants in the mitochondria. With mitochondrial health essential for fertility and early pregnancy fetal development, this is an important nutrient for conception and 1st trimester health. It is also a cofactor of several enzymatic reactions associated with bone and joint formation, as well as carbohydrate, protein and fat metabolism. Deficiency is associated with skeletal deformations, as well as gestational diabetes. Manganese is a cofactor in the formation of Hyaluronic Acid, and thus important in late term prenatals as well. Dosage preconception - 2nd trimester: 2-3mg Dosage 3rd trimester: 3-5mg Molybdenum: Molybdenum is a a cofactor in several enzymes associated with antioxidants. It is also a cofactor of iron metabolism and function, so can help with prevention of anemia. It can inhibit copper and thus because of the connection between excess copper and postpartum depression, molybdenum in a late term and lactation prenatal may be good addition. I look for lower levels of molybdenum, as it is a heavy metal and too much also be an issue. Dosage: 0-50mcg but never to exceed 100mg Potassium: Potassium is an electrolyte mineral. It is necessary for muscles to work properly. During pregnancy electrolyte needs go up to account for amniotic fluid and blood volume, and adequate amounts are need for that big 'ole muscle the uterus to function properly. In addition edema at the tail end of pregnancy can be associated with electrolyte imbalances. Magnesium is necessary for the balance of Potassium and Sodium in the blood and cells. Some research shows that higher levels of serum potassium in the early stages of pregnancy INCREASE the risk of gestational diabetes and preeclampsia. I believe this is more likely due to magnesium deficiency, and a lack of this necessary transport mineral causing a buildup of potassium in the blood stream, more so than an over consumption of potassium. Either way, I like to see Potassium in a prenatal, and very few have it. According to the HANES report, 97%of American fall short on Potassium intake. Dosage: 0-100mg (potassium iodide also provides potassium) Sodium: This is another important electrolyte in the production of amniotic fluid and blood volume. Of all the minerals in the diet, sodium is the one that Americans seem to get plenty of, in fact 90% of Americans OVER CONSUME sodium. In the modern, American diet, there is no need for a prenatal to contain sodium. Dosage: 0mg (no need for sodium in a prenatal) Phosphorus: This mineral is important for the health of bones, muscle contractions, and blood clotting. All things that are very important for pregnancy (especially during labor.) You will be hard pressed to find a prenatal that has phosphorus in it. Why? Because we generally get more than enough from our diet. Dosage: 0mg Boron: This is another trace mineral that you can sometimes come across in a prenatal. It is primarily there it aid in the absorption of Calcium, Magnesium and other minerals. It is also needed for your body to convert sunlight into Vitamin D naturally. Is it necessary in a prenatal? Not really. We need just a smidgen of boron in the diet, and we tend to get enough in the diet if we are eating brassica vegetables such as broccoli and Brussels sprouts. Dosage: 0-1mg Co-enzyme Q10: This is not something many of you have seen in a prenatal, but it is a nutrient that I think should be in them, especially in those marketed for conception and the first trimester. Co-enzyme Q10 plays a role in the body's metabolism of food into energy, and mitochondrial health. Amniotic Co-enzyme Q10 levels have been linked with adverse obstetrical outcomes, and amniotic levels of CoQ10 naturally rise throughout pregnancy. Research supports CoQ10 in helping encourage healthy ovaries, and in turn healthy embryos. Dosage: 50-100mg DHA: DHA has become the prenatal nutrient of the hour. DHA is super important for fertility and the neurological development of your baby. But it doesn't belong in a prenatal vitamin. DHA is a really great, and essential nutrient, for conception and the majority of pregnancy, but it can become an issue as you come into labor. I always recommend patients stop their DHA supplements the last month of labor. If you haven't heard, there has been a staggering rise in the number of postpartum hemorrhaging cases and deaths associated with PPH in the US. In correlation there has been an increase in the supplementation of DHA in pregnancy. Now, DHA use is not the primary cause of PPH, by any means, but it increases the risk. DHA is an anticoagulant. It blocks the receptor that Thromboxane A2 (the blood clotting agent produced in labor) attaches to in the uterus to stop bleeding as the placenta detaches. Excessive consumption of DHA can increase bleeding. I personally recommend a separate DHA to be taken preconception (unless threatened miscarriage), through about 36 weeks. Dosage: 0mg in a prenatal vitamin Dosage: 200-500mg (stopped at 36-37 weeks gestation, and started again after birth) Other Nutrients: I've seen a staggering list of other ingredient, such as herbs added to prenatal vitamins. I am not a big fan of this as not everyone responds to or needs herbal therapy. For example: Inositol is great for PCOS conception and pregnancy as it helps regulate insulin, but not everyone needs this. Herbs, such as milk thistle, and raspberry leaf are great, but again this is best taken separately. You can only put so much in a pill and have it be effective. The Take Home - Prenatal Do's and Don'tsI bet you are all asking yourselves (and me), "So what is a good prenatal brand?" Because everyone is so different, and everyone's needs are so different, I wish I could say, "THIS ONE! This is the one everyone should be taking," that's just not the case. I do have my favorites that I bounce around between based on patient needs. What I can show you is what NOT to take.
In the end supplements are a protector. They are are not meant to take over for your diet, and you can't expect a supplement to make up for a poor diet. RDA recommendations are the MINIMUM at which we need daily for survival, not overall function! Everyone's needs are different. You need to analyze your diet, your risks, your genetics and have a prenatal vitamin that fits your needs. Speaking with a professional trained in prenatal/maternal nutrition can help you better make this decision.
6 Comments
Hi! Thank you so much for your post. I just found out I’m pregnant and I can’t find a prenatal without all of the “dont’s” you listed. I’m super particular and have done a lot of research to make sure I find the right one. But I’m really stressing out. 11/3/2020 08:44:09 am
Hi Alena,
Britney
7/23/2024 07:32:35 pm
NATURAL HERBS IS THE REAL DEAL IN CURING HERPES-1&2, HIV/AIDS, HPV AND CANCER...Contact Dr Osato to get the natural herbs to cure yourself from that horrible disease/virus. I got the herbs from Dr Osato and I made use of it with the instructions he gave to me on how to use the natural herbal product, after usage I went for a checkup and my result was Negative and all the symptoms of herpes were completely gone from my body. I was cured from herpes-1&2 after using Dr Osato natural herbal medicine. You can contact Dr Osato on his email: [email protected] or WhatsApp +2347051705853 to get the herbal medicine from him and his website is https://osatoherbalcure.wordpress.com.
mark hold
7/4/2024 05:22:22 pm
One faithful day as i was watching a video on you tube i saw a comment of one MR PAUL HAVERSACK testifying of this great herbal healer doctor Moses Buba, That helped him enlarge his manhood .i was shocked and happy, so i quickly visited his website and emailed him within 30 mins he got back to me and told me all i need to buy and i did so after 4 days i received his herbal medicine ,he gave me instructions on how to use it ,as i am speaking to you people now after using the cream for just two weeks my manhood size is 10 inches long and 8.0 girth ,,am so happy and grateful for his work in my life thank you so much Doctor Moses buba ,,i also learnt he has cure for LOW SPERM COUNT,PREMATURE EJACULATION,ERECTILE DYSFUNCTION,HIV/AIDS VIRUS,DIABETES 1/2,HERPES DISEASE, CANCER, and lots more
Cheryl
7/11/2024 07:42:02 pm
My name is Cheryl Floyd. I am the happiest woman on the face of this earth. I am happy because of this man, a great spell who made my dreams come true. This is the handwork of Doctor Odunga. I contacted this man to help me save my marriage. My husband and I have been living without a child for 17 years and this has made me sort help in spells. I contacted Doctor Odunga and only him out of three spell casters did his work for me within 48 hours as he promised and I became pregnant with twins. I have been wanting to write this testimony for so long now when I became pregnant but I waited for the babies to be delivered and I am now a mother of twins, a boy and a girl. What else are you waiting for? Do you want a spell for pregnancy and solve fertility problems? Contact Doctor ODUNGA now at Email: [email protected] OR Whats App/Call +2348167159012 and he will talk to you directly.
Britney
7/23/2024 07:32:18 pm
NATURAL HERBS IS THE REAL DEAL IN CURING HERPES-1&2, HIV/AIDS, HPV AND CANCER...Contact Dr Osato to get the natural herbs to cure yourself from that horrible disease/virus. I got the herbs from Dr Osato and I made use of it with the instructions he gave to me on how to use the natural herbal product, after usage I went for a checkup and my result was Negative and all the symptoms of herpes were completely gone from my body. I was cured from herpes-1&2 after using Dr Osato natural herbal medicine. You can contact Dr Osato on his email: [email protected] or WhatsApp +2347051705853 to get the herbal medicine from him and his website is https://osatoherbalcure.wordpress.com Leave a Reply. |
 RSS Feed
RSS Feed